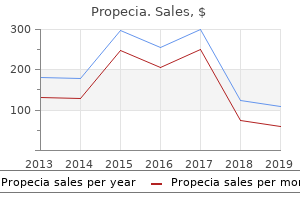
"Buy cheap propecia 1mg, hair loss cure september 2013."
By: Michael A. Gropper, MD, PhD
- Associate Professor, Department of Anesthesia, Director, Critical Care Medicine, University of California, San Francisco, CA

https://profiles.ucsf.edu/michael.gropper
The cost of relying on the large Hilbert space of an oscillator is that the sensitivity to hair loss in men kids discount propecia 1 mg on-line these interactions increases rapidly for macroscopic superposition states [11] hair loss in men shampoo purchase propecia 5 mg on line. Phase noise is treated in a similar manner hair loss cures purchase 1 mg propecia mastercard, introducing a phase scattering process with the bath to compute its e? This allows us to solve for the evolution of the density matrix of the resonator given some spurious process. We can write down a Lindblad equation to describe this evolution of the resonator under this interaction [35] as d? Therefore, T2 T1, even though energy decay is the only decoherence mechanism present! In this case, the interaction with the bath does not exchange resonator photons between the modes (as in the case of energy decay). It turns out that superpositions of coherent states have an interesting consequence for photon-loss mechanisms too [99]. Parity measurements therefore, can act as a photon-loss error detector, without collapsing the state since |? However, the two-legged cat [11] can only encode a classical bit of information (whether the parity is +1 or -1). To encode a quantum bit, each parity subspace needs to contain an entire logical Bloch sphere [99]. One basis that can encode superpositions within a parity subspace are four-legged cats. Because our logical states are chosen in the even parity subspace, all logical states have only even Fock weights [11], as X |? L Detecting any of these error states will indicate that an error has occurred in the memory. To see how errors can be decoded, consider the action of the annihilation operator 3. The Wigner function of the logical states |0iL (blue star) and |1iL are shown for |? However, a second photon loss even leads to an undetected error, since the state is back in the logical basis but at a new point on the logical Bloch sphere. Consequently, our state is never destroyed by photon loss, though the deterministic energy loss still occurs at rate. Although encoding a qubit state onto a four-legged cat has been achieved [68], universal control over a logical cat-qubit, for instance using the techniques in [69], is an important next step for the scheme. Finally, putting all of these pieces together, and showing overall gains in qubit performance, will be an incredible triumph. On their own, res M onators can serve as a test bed for studying material losses [101?104]. Coupled to superconducting qubits, low-loss resonators can act as quantum memories [52, 75, 107] or as buses for exchanging quantum information between qubits [57, 58]. This thesis is primarily concerned with one of these applications in particular, the quantum memory performance of a resonator. Therefore, we begin this chapter by presenting a generalized framework for to describe how loss mechanisms a? With that context, we present the design and development of a suite of low-loss microwave resonators and discuss the challenges and opportunities of a number of resonator geometries. This chapter culminates in the discovery of a viable technique for achieving state-of-the-art quantum memory performance for a superconducting-qubit-coupled device [52]. In practice, all circuit elements have some complex impedance that is neither completely capacitive nor inductive. Further, the concept of electromagnetic resonance is much more general than parallel or series circuits. The second observation that allows us to write down the quantum mechanical description of such a system is the treatment of boundary conditions [14]. Each resonator has a particular set of boundary conditions that forces these wave equations to a set of discrete eigenmodes. A given distribution of electromagnetic energy can be written as a sum over these modes [14], such that X?
Although good results have been reported after such surgery in a small number of cases hair loss cure quick effective propecia 1 mg, the potential risks to hair loss after childbirth generic propecia 5 mg mastercard the mother both during the pregnancy and in subsequent confinements should not be underestimated hair loss cure jo buy generic propecia 5 mg online. In the presence of a defective diaphragm, there is herniation of the abdominal viscera into the thorax at about 10?12 weeks, when the intestines return to the abdominal cavity from the umbilical cord. However, at least in some cases, intrathoracic herniation of viscera may be delayed until the second or third trimester of pregnancy. However, in about 50% of affected fetuses there are associated chromosomal abnormalities (mainly trisomy 18, trisomy 13 and Pallister?Killian syndrome mosaicism for tetrasomy 12p), other defects (mainly craniospinal defects, including spina bifida, hydrocephaly and the otherwise rare iniencephaly, and cardiac abnormalities) and genetic syndromes (such as Fryns syndrome, de Lange syndrome and Marfan syndrome). Diagnosis Prenatally, the diaphragm is imaged by ultrasonography as an echo-free space between the thorax and abdomen. Diaphragmatic hernia can be diagnosed by the ultrasonographic demonstration of stomach and intestines (90% of the cases) or liver (50%) in the thorax and the associated mediastinal shift to the opposite side. Herniated abdominal contents, associated with a left-sided diaphragmatic hernia, are easy to demonstrate because the echo-free fluid-filled stomach and small bowel contrast dramatically with the more echogenic fetal lung. In contrast, a right-sided hernia is more difficult to identify because the echogenicity of the fetal liver is similar to that of the lung, and visualization of the gall bladder in the right side of the fetal chest may be the only way of making the diagnosis. Polyhydramnios (usually after 25 weeks) is found in about 75% of cases and this may be the consequence of impaired fetal swallowing due to compression of the esophagus by the herniated abdominal organs. The main differential diagnosis is from cystic lung disease, such as cystic adenomatoid malformation or mediastinal cystic processes. In these cases, a fluid-filled structure causing mediastinal shift may be present within the chest. However, in contrast to diaphragmatic hernia, the upper abdominal anatomy is normal. Antenatal prediction of pulmonary hypoplasia remains one of the challenges of prenatal diagnosis because this would be vital in both counselling parents and also in selecting those cases that may benefit from prenatal surgery. Poor prognostic signs are, first, increased nuchal translucency thickness at 10?14 weeks, second, intrathoracic herniation of abdominal viscera before 20 weeks, and, third, severe mediastinal compression suggested by an abnormal ratio in the size of the cardiac ventricles and the development of polyhydramnios. Prognosis In the human, the bronchial tree is fully developed by the 16th week of gestation, at which time the full adult number of airways is established. The alveoli continue to develop even after birth, increasing in number and size until the growth of the chest wall is completed in adulthood. The growth of blood vessels supplying the acinus (intra-acinar vessels) parallels alveolar development, while the growth of pre-acinar vessels follows the development of the airways. In diaphragmatic hernia, the reduced thoracic space available to the developing lung leads to reduction in airways, alveoli and arteries. Furthermore, there is an increase in arterial medial wall thickness and extension of muscle peripherally into the small pre-acinar arteries, offering an explanation for the pulmonary hypertension and persistent fetal circulation observed after neonatal repair. Thus, although isolated diaphragmatic hernia is an anatomically simple defect, which is easily correctable, the mortality rate is about 50%. The main cause of death is hypoxemia due to pulmonary hypertension, resulting from the abnormal development of the pulmonary vascular bed. Fetal therapy Extensive animal studies have suggested that pulmonary hypoplasia and hypertension due to intrathoracic compression are reversible by in utero surgical repair. However, such therapy is likely to have limited success in the human because the bronchial tree is fully developed by the 16th week of gestation. For a fetus with a sonographically demonstrable large diaphragmatic hernia at 16?18 weeks, irreversible maldevelopment of the bronchial tree and vasculature is likely. However, in fetuses with a diaphragmatic defect which allows the intrathoracic herniation of abdominal viscera only after mid-gestation (when the bronchial tree and pre-acinar vessels are fully developed), prenatal correction, by allowing further development of the alveoli and intra-acinar vessels, may well prevent pulmonary hypoplasia and neonatal death. In a few cases of diaphragmatic hernia, hysterotomy and fetal surgery have been carried out but this intervention has now be abandoned in favor of minimally invasive surgery. Animal studies have demonstrated that obstruction of the trachea results in expansion of the fetal lungs by retained pulmonary secretions. Endoscopic occlusion of the fetal trachea has also been carried out in human fetuses with diaphragmatic hernia, but the number of cases is too small for useful conclusions to be drawn as to the effectiveness of such treatment. Prognosis Irrespective of the underlying cause, infants affected by pleural effusions usually present in the neonatal period with severe, and often fatal, respiratory insufficiency. This is either a direct result of pulmonary compression caused by the effusions, or due to pulmonary hypoplasia secondary to chronic intrathoracic compression. The overall mortality of neonates with pleural effusions is 25%, with a range from 15% in infants with isolated pleural effusions to 95% in those with gross hydrops.
Some tion to hair loss in men 100 cheap 1mg propecia sampling the mesentery for lymph nodes hair loss endocrinologist purchase propecia 1 mg line, specimens may be so distorted that they cannot submit sections of mesenteric blood vessels and be easily opened and pinned? The initial step is to hair loss in men gold order propecia 1mg free shipping identify the structures that are present in the re sected specimen. The large intestine is readily Specimen Photography distinguished from the small intestine by its larger diameter and the presence of longitudinal Photographs of the specimen should be liberally muscle bands (the teniae coli), sacculations (the taken to document further the gross? In addi pecially the distribution and nature of the muco tion, the small intestine shows mucosal folds that sal alterations. Photograph the specimen after it stretch across the entire circumference of the has been opened and? Photographs of the bowel, whereas the mucosal folds of the large in unopened bowel are generally useless. Several features may tends to both accentuate the mucosal alterations be helpful in appreciating the various regions and reduce the amount of re? The cecum is usually quite Always position the specimen anatomically on apparent, and it can be used to identify the origin the photography table. The transverse colon ample, should be positioned so that the ascending can be recognized by its large mesenteric pedicle colon is to the anatomic right, the descending attachment, while the sigmoid colon has a rela colon is to the left, and the transverse colon is tively short mesenteric pedicle. Non-Neoplastic Intestinal Disease 69 of rectum is included in the specimen, it can be Remember to section all regions of the bowel distinguished from the sigmoid colon by the by using a method of stepwise sectioning at regu absence of a peritoneal surface lining. As de pling of representative lymph nodes from each scribed previously, these soft tissues should be level will suf? Sampling of the mesentery removed according to their anatomic location, should also include a section of the mesenteric and each portion should be clearly labeled so blood vessels and sections of any focal lesions. Remember, most of the lymph nodes Your Surgical Pathology Report on are found at the junction of the bowel and mesen Non-Neoplastic Intestinal Disease teric fat. Open the bowel along its entire length, cutting the small bowel along its mesenteric at-. Polaroid or digital photograph of the entire Record the number of lymph nodes examined specimen, so that the sites from which histologic and the presence or absence of lymph node sections were taken can be indicated on the metastases. The median section should demonstrate the largest cross-sectional area of the head of the polyp, its interface with the stalk, and the Polyps of the gastrointestinal tract are usually surgical margin. The importance of trisecting removed endoscopically by a single incision at the polyp is readily apparent if one pauses to the base of the polyp stalk. Although these speci consider the impact of this method on the his mens lack the size and complexity of more tologic sections. Serial sections into the median extended bowel resections, they are delicate section of a trisected polyp will approach the structures that require meticulous processing. The polypectomy specimen poses three Important Issues to Address important questions to the surgical pathologist: (1) Are adenomatous changes present? Measure the height or absence of invasion of the stalk and of the and diameter of the polyp. Next, place the speci submucosa at the base of the stalk or base of men in formalin for? As illustrated, this relation from the deepest part of the invasive carcinoma ship is usually best demonstrated by trisecting component to the nearest polyp margin. Does the polyp into two lateral caps and one median the adenomatous epithelium or the in? As is true for other speci invasion that serves as the key feature for as mens, a systematic approach to your dissection is sessing T? when staging the tumor. Multiple the best way to ensure that all of the appropriate cancers should be looked for, described, and information is included in your? Next, iden bowel perforation (a hole in the bowel wall) is tify the segment of bowel that was resected, and associated with the tumor. The soft tissue margin is only important tine shows mucosal folds that stretch across the for rectal cancers and for colon cancers located entire circumference of the bowel, whereas the on the mesenteric aspect of the bowel.
An echogenic linear structure can be visualized by ultrasound in the dilated common bile duct hair loss in men jogger buy propecia 1mg without prescription. It is a progressive painless jaundice that occurs in elderly persons hair loss 5 months after giving birth propecia 1mg amex, accompanied by important weight loss hair loss cure 54 generic propecia 1 mg on-line. On ultrasound, the intrahepatic bile ducts are dilated, the common bile duct is significantly enlarged (15-25 mm), and the ultrasound Courvoisier-Terrier sign is present (Figs. It generates progressive painless obstructive jaundice that frequently shows few symptoms. It may be accompanied by moderate anemia (the tumor can ulcerate into the duodenum, with occult bleeding). Ultrasound shows dilated intrahepatic bile ducts, an enlarged common bile duct along its entire length, a distended gallbladder. A mild or moderate dilatation of the duct of Wirsung (through a Wirsung obstruction) is also common. Ampulloma can be benign or malignant and its differentiation is made by histological biopsy. Therapy includes endoscopic or surgical ampullectomy or endoscopic prosthesis placement. The ultrasound examination of the common bile duct will reveal its compression by a large, frequently inhomogeneous cephalic pancreas, with calcifications, or by a pancreatic head pseudocyst (anechoic 116 hesion with hyperechoic walls). This visualizes the intra and extrahepatic bile ducts and at the same time, it evaluates the pancreas and the liver. In this chapter, we presented the clinical and imaging approach to a jaundice syndrome. The type of jaundice, hepatocellular or obstructive, can be established by ultrasound. In hepatocellular jaundice, ultrasound can provide some diagnostic but not very relevant elements. In a retrospective study, performed in the Ultrasound Department of the Timisoara County Hospital several years ago, by analyzing 77 obstructive jaundice cases, the etiology of obstructive jaundice could be clearly established by transabdominal ultrasound in 57. Subsequently, the same study was conducted prospectively in a group of 46 obstructive jaundice cases and etiologic diagnosis by ultrasound was made in 73. These data are in accordance with most published data that indicate a 60-80% sensitivity of ultrasound in the etiologic diagnosis of obstructive jaundice. Regarding the frequency of different causes of obstructive jaundice, in the above mentioned study we found that 44. In conclusion, we must mention that the experience, the theoretical and practical skills of the examiner, the type of ultrasound machine used, as well as the commitment to the task of clarifying the etiology of jaundice are extremely important. Situated in the splenic loge, the spleen is an organ with a parenchymal structure, with similar echogenicity to that of the liver. The spleen is evaluated by ultrasound either through left intercostal sections or through sections below the left costal margin. For inexperienced ultrasonographists it is relatively difficult to include the entire spleen in a single section, particularly in splenomegaly cases. The beginner tends to include only a portion of the spleen in the ultrasound section, which makes its accurate measurement impossible. The examination of the spleen will be conducted in such a manner as to include both splenic poles in the ultrasound plane, allowing accurate measurement. Under pathological conditions, the spleen echogenicity may be modified, but it is almost impossible to speculate regarding the hematological or hepatic cause based only on the spleen structural and echogenicity changes. From a clinical point of view, the spleen assessment is valuable in hematologic or liver diseases, in some infectious diseases, after abdominal trauma or surgery, as well as in prolonged fever. Splenomegaly Definition: an enlargement of the spleen exceeding 12 cm in its long axis. Some authors consider a normal spleen size up to 11 cm, others, up to 13 or even 14 cm, but most ultrasonographists consider the value of 12 cm as being the upper limit of normal.
The authors speculated that this increase in common carotid artery velocity reflected increased cardiac output associated with fetal anemia hair loss in men xmas purchase 5 mg propecia, rather than a chemoreceptormediated redistribution in blood flow hair loss weight gain generic propecia 1 mg without a prescription, as seen in hypoxemic growth-restricted fetuses 27 hair loss in men 91 cheap propecia 5 mg free shipping. In an extended series of 95 previously untransfused fetuses undergoing cordocentesis for rhesus disease, there was a significant association between the increase in mean velocity in the middle cerebral artery with the degree of fetal anemia 16. In an additional series of 212 fetuses that had a transfusion 2?3 weeks previously, the relation between blood velocity and anemia was weaker 16. In a prospective study of 16 fetuses from isoimmunized pregnancies, they found that all the anemic fetuses had peak velocity values above the normal mean for gestation, whereas none of the fetuses with peak velocity below the normal mean was anemic 28. On the basis of these results, they suggested that, in the management of isoimmunized pregnancies, the indication for cordocentesis should be a peak systolic velocity above the normal mean for gestation. These results were confirmed in a multicenter study involving 111 fetuses from isoimmunized pregnancies; all moderately or severely anemic fetuses had increased peak velocity in the middle cerebral artery 29. Furthermore, there was a good correlation between delta peak velocities and delta hematocrits for the first procedure. The deceleration angle between the line describing the average slope during the diastolic phase of the cycle and the vertical axis was measured and expressed in multiples of the median (MoM) for gestational age. A decrease in the deceleration angle was associated with fetal anemia and, at a threshold deceleration angle of < 0. It was concluded that all cases of severe anemia could be identified before the development of hydrops, and, if, in the management of red cell isoimmunization, cordocentesis is only carried out if the deceleration angle is < 0. Figure 2: Blood velocity in the fetal thoracic aorta (left) and middle cerebral artery (right) in red cell isoimmunized pregnancies plotted on the appropriate reference range (mean, 95th and 5th centiles) for gestation. The findings of increased blood velocity in the fetal arteries with anemia (Figure 2 and Figure 3) are compatible with the data from the fetal cardiac Doppler studies. If it is assumed that, in anemia, the cross-sectional area of the fetal descending aorta and middle cerebral arteries does not change, the increased velocity would reflect an increase in both central and peripheral blood flow due to increased cardiac output. The decreased aortic velocity in some hydropic fetuses may be the consequence of cardiac decompensation, presumably due to the associated hypoxia and lactic acidosis and to the impaired venous return due to liver infiltration with hemopoietic tissue 2. Figure 3: Flow velocity waveform in the fetal middle cerebral artery in a severely anemic fetus at 22 weeks (left) and in a normal fetus (right). In fetal anemia, blood velocity is increased Blood velocity in fetal veins Rightmire et al. Although the velocity was higher than in non-anemic controls, there was no significant correlation with fetal hematocrit. In the same study, the intrahepatic umbilical venous velocity was not significantly different from non-anemic controls. It was postulated that the increased flow was the result of reduced blood viscosity due to the reduced hematocrit. They concluded that pregnancies with a mild or no history of fetal anemia may be monitored by a combination of serial antibody quantification and Doppler measurement of umbilical vein maximal flow velocities. It was suggested that the increase in ductus venosus blood flow in anemic fetuses reflects increased venous return and therefore cardiac preload. Furthermore, this study showed that heart failure is not the primary mechanism for the development of hydrops, but rather the end-stage of severe anemia, because the pulsatility of venous blood flow waveforms was not increased. Hydrops may be due to reduced colloid osmotic pressure, hypoxia-induced endothelial damage and increased permeability. Severe fetal anemia, with consequent cardiac failure, is associated with a reversed a? wave in the ductus venosus. Under these conditions, pulsations are also present in the venous portal system (which in normal fetuses is characterized by a continuous flow). The pulsatile pattern present in the venous system corresponds to findings in children with portal hypertension 36. Since, in fetal anemia, resistance to flow in the fetal circulation and placenta is unchanged, an increase of umbilical venous blood flow is in accordance with high cardiac output and elevated arterial velocities. It was suggested that the gradual decrease in flow, coinciding with resolution of fetal ascites, was the result of absorption of the transfused blood and correction of the fetal anemia. Doppler studies of impedance to flow in the umbilical artery before and soon after intravascular top-up transfusion provided conflicting results. It was postulated that simple needling of fetal blood vessels stimulates a humoral vasodilator mechanism. Supportive evidence was provided by the finding that fetal blood levels of vasoactive substances with vasodilatatory effects, like prostaglandins and atrial natriuretic peptide, are increased after an intravascular blood transfusion 39,40. There was a significant decrease in mean blood velocity in both the descending thoracic aorta (Figure 4) and common carotid artery.
Buy discount propecia 1mg line. Hair Loss after extreme weight loss.
References:
- http://nexusacademicpublishers.com/uploads/files/Nexus_191.pdf
- https://dese.mo.gov/sites/default/files/aged-Animal-Repro-Student-Ref..pdf
- https://www.who.int/selection_medicines/list/WMF2008.pdf